


showCASE No. 92 | How to heal the Polish healthcare system
How to heal the Polish healthcare system?
By: Izabela Styczyńska, Vice President of CASE Management Board and Agnieszka Kulesa, CASE Economist
Diagnosis[1]
Ageing of societies, increasing share of expenses related to the treatment of chronic diseases in the healthcare expenditures, and social expectations to have a quick access to new medical technologies are among the main factors that necessitate search for new solutions in the healthcare sector across Europe. Poland is no exception. Regrettably, however, while several other European countries base their decisions and actions on solid evidence-based healthcare diagnosis,[2] in Poland the Ministry of Health has never performed a complex analysis of the functioning of the healthcare sector. Existing studies are of a fragmentary nature, refer to individual elements of the system, and are not aimed at identifying complex challenges ahead of the healthcare sector, despite the fact that WHO already in 2004 stressed the need to support all decisions in the sector by evidence-based research. The process of comprehensive diagnosis is important, since Poland struggles with several structural challenges in the healthcare sector, which make the system inefficient in the short term, and potentially paralyzed in the long term. The most pressing challenges include:
Misallocation of resources
One of the main problems in all the developed countries is an unsatisfactory level of financing devoted to the healthcare sector. In Poland, expenses on the sector nominally increased more than twice between 2006–2016, and by 69% in real terms. Despite this fact Poland remains a country where the share of healthcare expenditures in GDP, as well as per capita, is one of the lowest in Europe (p. 24). On the top of that, as the Organisation for Economic Co-operation and Development (OECD) health statistics show, the allocation of limited financial resources is very inefficient.
Poland is a country where hospital-centric allocation of funds in one of the highest, just after Greece. Financing of effective preventive measures that would allow to detect diseases at their earliest stages is insufficient, to say the least. This, in turn – combined with an underestimated role of the outpatient care – results in greater demand for hospitalisation and leads to greater expenditures in the most cost-intensive section of the whole healthcare system. Indeed, currently Polish hospitals absorb 36% of current spending on health (the OECD average is 28%). Moreover, in years 2004–2017 the share of hospital treatment in the expenditures of the National Health Fund (Narodowy Fundusz Zdrowia, NFZ) has increased from 43.4% to over 50%. The lack of effective disease prevention and health promotion will most likely have broad and long-term impacts. The World Health Organization perceives noncommunicable diseases, such as diabetes, cancer and heart disease, as one of the top ten threats to global health in 2019 and beyond. Among the five major risk factors are physical inactivity, unhealthy diets and air pollution. Moreover, cardiac diseases caused 46% of all deaths in Poland in 2013, and 610.5 deaths per 100,000 inhabitants caused by circulatory diseases were noted in 2015 (with the EU average of 381.4).
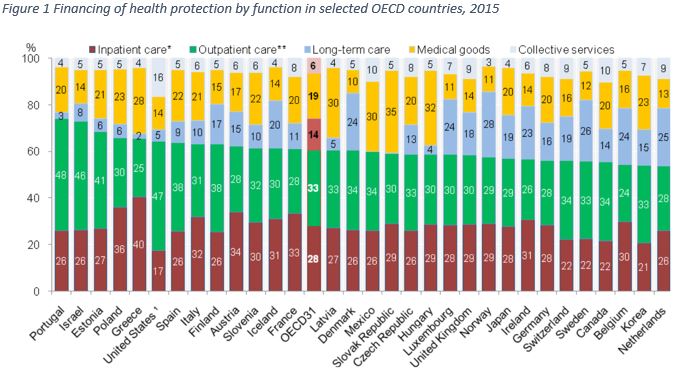
* Collective services include prevention, public health and system administrative costs
Source: Ch. Sowada, “Financing health system in Poland: spending levels and allocation of funds”, p. 27 (on the basis of: OECD (2017) Health Statistics 2017, WHO Global Health Expenditure Database), in: S. Golinowska et al., “What’s next for healthcare in Poland: diagnosis and prognosis”, mBank-CASE Seminar Proceedings No. 156/2018.
Workforce shortages
Already in 2006 the WHO alarmed that the majority of the European countries would have to deal with the problem of workforce shortages in the healthcare sector, with main challenges related to providing high-quality education, vocational education and training (VET), as well as maintenance of satisfactory salary. As a result, the EU has communicated several initiatives supporting employment in the healthcare sector (see for example: 2008 Green Paper on the European Workforce; 2012 Working Document on an Action Plan for the EU Health Workforce; 2013 Investing in Health Working Document; and WHO 2010 Global Code of Practice on the International Recruitment of Health Personnel).
Alas, no corresponding systemic programme to address the challenge of the future workforce shortages in the healthcare sector in a structural and comprehensive manner has been created in Poland thus far.[1] Moreover, Polish experts have been experiencing difficulties in assessing the real future needs of the healthcare workforce due to data constraints. As a result, existing data, studies and forecasts are fragmentary, and very often do not encompass such factors as demographic and epidemiologic trends (p.37). At the same time, those studies that have been produced thus far consistently show that human resources continue to be an Achilles heel of the Polish healthcare system. Presently, there are 5.2 nurses per 1,000 inhabitants in Poland (the OECD average is 9) and it is estimated that by 2035 this number will drop to 3.65. Moreover, the average age of a working nurses is now 51 years, and of doctors – 50 years, and both numbers are expected to rise in the near future. This, combined with the fast pace of aging of the population is forecasted to result in a shortage of 169,000 nurses and midwives within the next 11 years. At the same time, the government spending on health in Poland is one of the lowest in the EU28 and amounts to USD 1,352 per capita (only Latvia and Lithuania spend less).
Governance
The concept of good governance for health has been widely presented and discussed by many international organizations and experts (see for example this article by T. Chanturidze and K. Oberman, World Bank’s 2011 Governance in the Health Sector or WHO’s 2012 Governance for health in the 21st century). The concept is based on specific parameters, which should be satisfied in order to call the governance successful. The parameters are in turn related to such areas as: the formulation of health policy and strategic plans; generation of intelligence; presentation of health priorities, problems, and needs; the creation of incentives for different stakeholders; and the assurance of accountability and responsibility of diverse healthcare stakeholders. International organizations indicate that the weakness of governance in healthcare are observed in all European countries, and Poland is not an exception in this respect. Problems identified in Poland encompass, among others: long-term development of health workforce; ineffectiveness in supporting satisfactory financing; difficulties in the coordination of activities between diverse stakeholders and/or sectors; insufficient social dialogue; lack of institutionalised expert experience; and ‘gaps in the integration of successive stages in the medical treatment process’ (p. 11).
The topic of good governance is closely related to the issue of specific managerial skills required from the decision makers, which they oftentimes lack due to the specific and complex nature of this sector. Many international institutions (WHO included) implement study programmes and trainings for medical specialist in order to gain leadership skills and increase their economic and managerial competences. Unfortunately, such activities are not very popular in Poland.
Treatment
For the last couple of years all the challenges of the healthcare sector have been in the strategic agendas of several European countries and institutions at the EU level. For example, the investment approach to health is visible in the EU Health Programme that feeds into the overall Europe2020 strategy. Good health is perceived there as one of the prerequisites for a smart, sustainable and inclusive economy, and health of the society together with good functioning of the health services are treated as productive factors of growth and employment.
The concept of investing in health in Poland was supposed to be made operational through national health plans. Unfortunately, the plans that are being developed usually look better on paper than in practice. For example, the current plan covering years 2016–2020 provides a list of broadly formulated strategic goals – extending the number of years in health, improving the quality of life related to health, and limiting social inequalities as regards health –
but ‘in light of the short implementation period, they sound like particularly empty slogans’ (p. 49). What is most surprising is the fact that main health threats, such as circulatory system disease or cancer, have not been indicated in the plan as the main health problems requiring the states’ attention.
In addition, long-term policy defining growth of compensation in the healthcare sector is still lacking. As depicted in the Figure 2, salary increase of diverse groups of employees were mainly dependent on the number of strikes and protests by doctors and nurses rather than based on a well thought-through long-term programme, or a national strategy.
Figure 2 Analysis of the introduction of legal regulations in the area of growth of compensation in the healthcare system as a response to medical workers’ strikes and protests
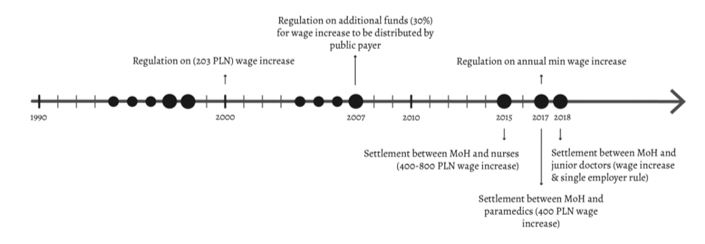
* The dots designate strikes and protests, and their size reflects the size of the protest
Source: A. Domagała, “Health workforce: personnel shortages and ways to overcome them”, p. 41 (on the basis of: K. Dubas-Jakóbczyk, A. Domagała, M. Mikos, “Impact of the doctor deficit on hospital management in Poland – a mixed methods study”, International Journal of Health Planning and Management, 2018, Volume 28, Issue suppl 4), in: S. Golinowska et al., “What’s next for healthcare in Poland: diagnosis and prognosis”, mBank-CASE Seminar Proceedings No. 156/2018.
Given that the expenses on remuneration are the biggest category in the healthcare sector budget, unplanned salary increases usually lead to financial deficits of hospitals and/or inefficient hospital management.
Conclusions
Continued attempts to respond to the demographic and economic challenges have been made by a number of European states in order to assure their citizens’ access to high quality healthcare and the right to effectively benefit from medical treatments. Sadly, Poland has not been one of them.
Statistics speak for themselves as regards the need for urgent action. In 2015 diseases of the circulatory system and cancer were the leading causes of death in the EU. People in Poland were among most affected by cancer with 304.5 deaths per 100,000 inhabitants (above the EU average of 261 deaths per 100,000 inhabitants). Existing studies show that in countries where preventive measures are introduced and cancer is diagnosed in its early stages, the survival rates are higher. Furthermore, according to Eurostat, life expectancy of Poles in 2017 was still six years below that in countries with the best results: Italy, Sweden, and Spain. Even more worryingly, 2018 was the second year in a row
in which the life expectancy in Poland declined. Ignoring the statistics and research results, the discussion in Poland continues to focus solely on increasing funding for the healthcare sector (and they were proudly announced by the Prime Minister M. Morawiecki), with no additional consideration for restructuring the healthcare system in a systemic and comprehensive way.
Secondly, despite the fact that all the international organizations highlight the need to undertake measures increasing the workforce in the healthcare sector, no dedicated strategy has been introduced in Poland so far. This is especially worrisome as Poland is a country with a significant threat of medical personnel shortages due to the increased migration of professionals (see for example this article on migration of the medical professionals, in Polish only) coupled with increasing demand for their services caused by the ageing of the population. Nevertheless, the number of proposed residencies fluctuates from year to year with no clear path supported by the thoughtful evidence-based division mechanisms. Similarly, no strategic moves have been introduced in order to secure decent and competitive salaries in the sector, encouraging young professionals to stay.
For now, new protests are foreseen in the healthcare sector, again just before the elections. What physicians advocate for is in fact not only higher remuneration, but also substantial structural changes to the system. What they seem to recognise is the fact that, as evidence shows, broadly understood investments in health bring returns to the health sector, other sectors, and the wider economy. Public health is not only about costs – it is about the society’s future and its general prosperity. The question remains, will the Polish policy makers finally behave in a responsible way and turn to strategic and systemic planning in support of rational investments in the healthcare sector?
[1] For example, the Polish Chamber of Physicians and Dentists produces analysis on the demand for doctors, such as this one, but their effects on policy are rather limited.
[1] This paper has been created on the basis of the mBank-CASE Seminar Proceedings No. 156/2018: S. Golinowska et al., “What’s next for healthcare in Poland: diagnosis and prognosis”.
[2] For more national examples for the UK, the Netherlands, or Sweden, please refer to the above-mentioned report.
By: Izabela Styczyńska, Vice President of CASE Management Board and Agnieszka Kulesa, CASE Economist